
This guide contains Amazon affiliate links. If you buy through them, the site may earn a small commission at no extra cost to you. Product mentions are based on published evidence and device specifications, not paid placement.
If a friend at the gym told you red light therapy for muscle recovery is the new edge, it is fair to ask whether the marketing has real science behind it. This guide is built from peer-reviewed photobiomodulation research, and it tries to be honest about both what the evidence supports and where it falls short.
The short version is more nuanced than either side suggests. For pre-exercise use, the evidence for reduced muscle soreness is meaningful, though rated low-to-moderate certainty. For late-phase delayed-onset muscle soreness (DOMS) at 72–96 hours, the effect is moderate. And for consumer LED panels matching the laser protocols used in most clinical studies, the evidence is weaker, which is worth understanding before you spend anything.
This guide covers what the research actually shows, how to choose a device honestly, and a practical protocol grounded in published evidence rather than influencer claims.
What Is Red Light Therapy (Photobiomodulation)?
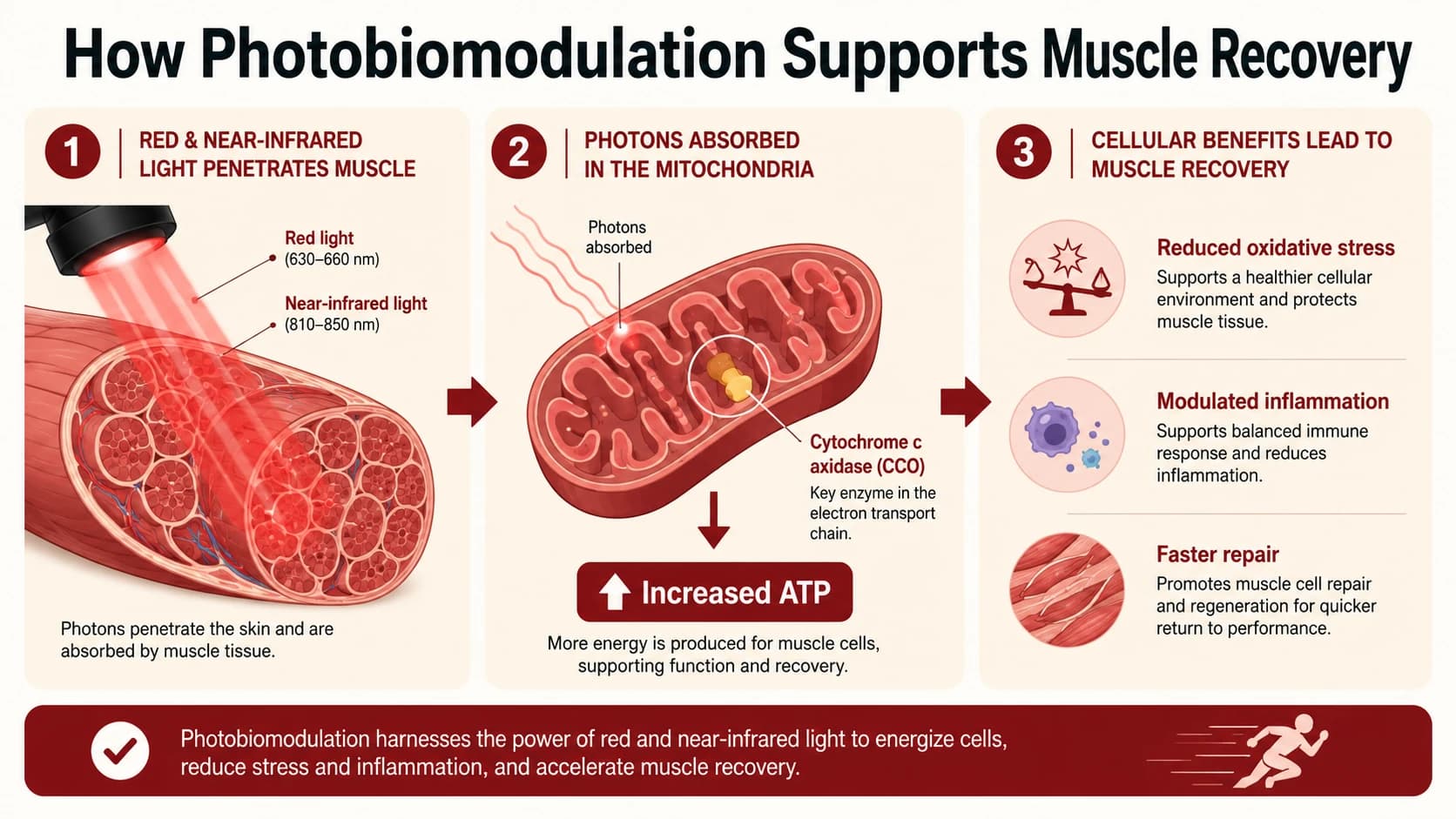
Red light therapy, formally called photobiomodulation (PBM), shines specific wavelengths of red and near-infrared light onto the body. It does not heat the tissue, does not break the skin, and has nothing to do with UV light or heat lamps. A 2024 review in the Journal of the American Academy of Dermatology (JAAD CME) explains that PBM uses red light (about 620–700 nm) and near-infrared light (about 700–1440 nm), and that the light is mainly absorbed by an enzyme inside the cell's mitochondria.
The mitochondrial mechanism
When red or near-infrared light hits this enzyme, the mitochondria, the cell's power plants, run a little more efficiently. The result is more energy (ATP), less oxidative stress, and a calming effect on inflammation signals. For a working muscle, that matters because the same power plants that tire out under load are the ones being nudged.
660 nm vs 850 nm — why dual-wavelength panels matter
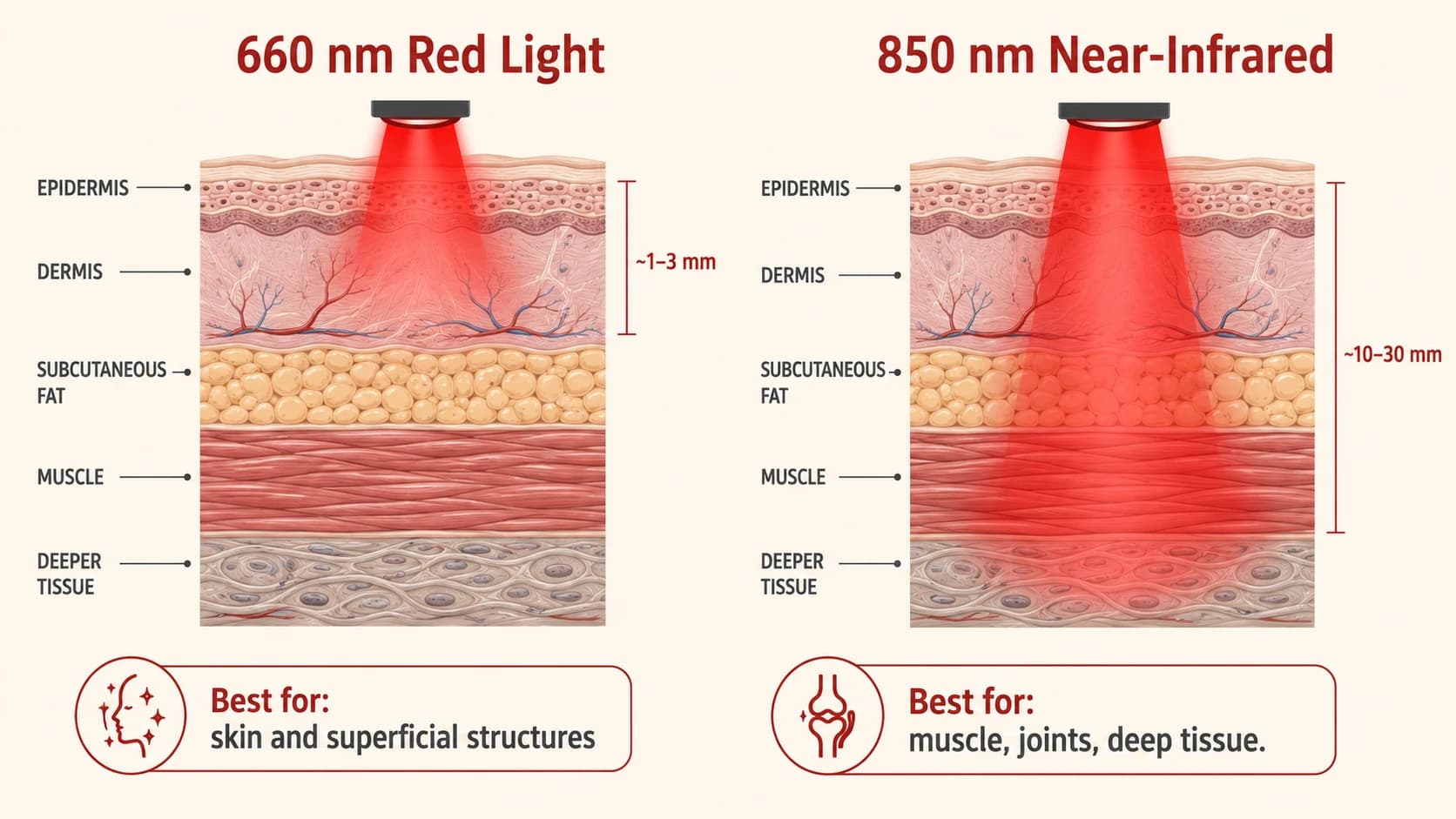
Wavelength sets the depth. 660 nm red light reaches only about 1 to 3 mm in, which suits skin and surface tissue. 850 nm near-infrared light goes much deeper, into the range where muscle sits. A 2024 review in the Journal of Functional Morphology and Kinesiology (Lawrence & Sorra, 2024) notes that the LED light in home panels does not reach as deep as the laser light used in clinics, an important point for anyone buying a consumer device.
What Does the Research Say About PBM for Muscle Recovery?
Pre-exercise application has the strongest evidence
A 2025 review that pooled 19 trials in 672 people found that red light applied before exercise meaningfully reduced muscle soreness (Canez et al., 2025). The authors rated the certainty as low, but the effect was consistent enough that using it before exercise has become the most-repeated finding in this area.
Recommended dosing for large muscle groups
The most cited dosing guidance comes from Leal-Junior, Lopes-Martins and Bjordal (PMC6546960). Their analysis of positive RCTs found doses in the 60–300 joules per session range produced beneficial outcomes for large muscle groups, with the most effective range narrowing to 120–300 J in more recent trials.
Performance and endurance
A 2024 review in J Funct Morphol Kinesiol (PMC11503318) concluded that pre-exercise LLLT shows beneficial effects on muscular performance, endurance, and reduced perceived fatigue. The same review was more cautious about acute deep-tissue injury, where evidence remains less convincing.
Red Light Therapy and DOMS — What the Evidence Shows
Delayed-onset muscle soreness peaks 24–72 hours after unfamiliar eccentric loading and usually resolves within 5–7 days. Two recent meta-analyses give a nuanced picture.
A 2025 network meta-analysis in the Journal of Pain Research (PMC12178262) found red light did better than a placebo at the 24-hour mark, ranking it among the more effective recovery methods studied — ahead of some alternatives like cold water immersion, whose evidence we review separately in our cold showers explainer.
A separate 2025 review (Tsou et al., 2025) of 14 trials found a different pattern: no clear effect on pain at 24 or 48 hours, but moderate effects at 72 and 96 hours. So red light seems most useful for the later part of the soreness curve, when applied after hard, muscle-damaging exercise.
What the Evidence Does NOT Yet Support (Honest Limitations)
Three things deserve to be said clearly.
Results are not universal. A randomized crossover trial in young untrained women (PMC8222918) found that 808 nm laser PBM at 28 J did not improve biceps brachii performance, RPE, or DOMS versus placebo. Sex, training status, and dose all moderate outcomes.
Most clinical trials used laser, not LED. Consumer panels sold on Amazon are LED-based. Per the 2024 J Funct Morphol Kinesiol review (PMC11503318), laser light is coherent and monochromatic and penetrates deeper than the non-coherent, broader-spectrum light from LEDs. That doesn't make LEDs useless — it means the at-home evidence base is weaker than the clinical one.
Certainty of evidence is low to moderate. Even the positive meta-analyses note low-to-moderate GRADE certainty, heterogeneous protocols, and a lack of standardized dosing. PBM is a useful adjunct, not a replacement for sleep, protein intake, and progressive training load.
How to Use Red Light Therapy for Muscle Recovery

Drawing the strongest threads from the studies above, here is a protocol that mirrors the positive RCTs:
| Variable | Practical guidance |
|---|---|
| When | 5–30 min before exercise (strongest evidence); secondary use within 1 hour post-workout |
| Wavelengths | Dual panel emitting both 660 nm + 850 nm |
| Distance from panel | 10–30 cm per manufacturer guidance (closer = higher irradiance) |
| Time per zone | 5–15 min per large muscle group |
| Target dose | ~60–300 J per zone (most effective range: 120–300 J) |
| Frequency | 3–5 sessions per week |
| Cycle length | Reassess after 4–6 weeks of consistent use |
Goggles are recommended whenever you're within a metre of a high-irradiance panel. Pregnant individuals, anyone on photosensitizing medications, and people with active skin cancers or photosensitivity disorders should consult a clinician first.
Best Red Light Therapy Devices for Muscle Recovery in 2025

After filtering Amazon's current options by wavelength quality (660 nm + 850 nm baseline), review depth, star rating, and brand transparency, here are the picks that hold up.
🏆 Editor's Choice: Hooga HG300 Red Light Therapy Panel
The HG300 is a commonly recommended starter-to-intermediate panel and a sensible benchmark for value. It combines 660 nm and 850 nm in a balanced ratio, with a built-in timer, cooling fans, and a kickstand for targeted muscle and joint work.
Honest limitations: Only the two core wavelengths. The cooling fan is audible. Like most consumer panels, it does not publish a third-party spectroradiometer report, so treat any irradiance figures as manufacturer estimates.
Best for: First-time buyers who want a proven, well-reviewed panel for targeted work.
🥈 Runner-Up / Best High-Power Panel: BestQool 105W Dual-Chip Panel
BestQool's dual-chip panel sits a rung up in output from the HG300, packing both 660 nm and 850 nm into each diode. A useful point in its favor is that the brand publishes third-party testing for several models, a transparency advantage few competitors match.
Honest limitations: Higher output shortens the recommended session length, so following the manufacturer's distance and time guidance matters more here. Two wavelengths only.
Best for: Athletes and lifters who want a higher-output panel without stepping into full-body pricing.
🌟 Best Value (Massive Review Base): Viconor 120 LED Panel
The Viconor uses a near-infrared-heavy ratio of 660 nm to 850 nm (roughly one red chip to two NIR chips per LED). That NIR-heavy profile favors deeper tissue, which is what you want for muscle recovery specifically, and the curved housing helps direct light toward the target zone. It is one of the more heavily reviewed budget panels in the category.
Honest limitations: Manufacturer irradiance numbers are not verified by third-party testing, so treat them cautiously. Build quality is acceptable rather than premium.
Best for: Budget-conscious buyers who want NIR-heavy output for muscle work.
Best Full-Body Panel: Hooga HG1500
If you want to treat large posterior-chain groups (back, hamstrings, glutes) in a single session, the HG1500 is Hooga's full-size option, combining 660 nm and 850 nm across a much larger panel to approximate a half-body session at home.
Honest limitations: Significantly more expensive than the HG300. Requires wall mounting or a dedicated stand for proper use.
Best for: Serious recreational and competitive athletes treating multiple muscle groups per session.
Best Compact Premium Panel: Mito Red Light – MitoMIN 2.0
Mito Red Light is one of the more established specialist brands in the space. The MitoMIN 2.0 is its compact panel, designed for face, neck, and targeted muscle zones, at a more accessible price than its full-size line. It uses 660 nm and 850 nm with clear documentation, which is a point in its favor for buyers who value transparency.
Honest limitations: Smaller treatment area, so it is best for spot work rather than large posterior-chain sessions, and pricing per area of coverage is on the premium side.
Best for: Buyers who prioritise brand transparency and documentation, treating shoulders, calves, or forearms.
Best Wearable Wrap for Targeted Recovery: Triple-Chip Red Light Wrap
A wrap is genuinely useful for muscle recovery in a way panels are not: you can apply 660 nm and 850 nm directly to a specific muscle (lower back, quad, hamstring) while sitting on the couch. This triple-chip wrap delivers both wavelengths in a portable belt format with adjustable straps.
Honest limitations: Coverage is fixed by the wrap's dimensions, so it is less flexible than a panel, and battery life limits how long each session can run.
Best for: Athletes and desk workers who want hands-free, targeted recovery on specific muscle groups.
Best Budget Multi-Mode Panel: SUBRUN Dual-Chip Panel
The SUBRUN dual-chip panel offers three operating modes (red-only, NIR-only, combined) at an accessible price. The dual-chip design means each LED emits both 660 nm and 850 nm.
Honest limitations: A newer listing with limited long-term durability data, so verify current pricing and reviews before committing.
Best for: First-time buyers testing the modality at minimum financial risk.
Honorable Mentions
SCESFU E300 60-LED Panel (Buy on Amazon) — Three-mode 660/850/combined panel with a built-in timer. A reasonable second-tier budget option.
Hooga Red Light Therapy Wrap (405 LED) (Buy on Amazon) — A higher-LED-count alternative to the featured wrap, but its review base is still thin and mixed at the time of writing, so it is worth waiting for more reviews before buying.
Device Comparison Table
| Device | Wavelengths | Format | Best for | Buy |
|---|---|---|---|---|
| Hooga HG300 | 660 + 850 nm | Panel | Proven starter panel | Buy Now |
| BestQool | 660 + 850 nm | Panel (dual-chip) | Higher output, third-party tested | Buy Now |
| Viconor | 660 + 850 nm (NIR-heavy) | Panel | Budget, NIR-heavy for muscle | Buy Now |
| Hooga HG1500 | 660 + 850 nm | Full-body panel | Treating large muscle groups | Buy Now |
| Mito MitoMIN 2.0 | 660 + 850 nm | Compact panel | Documentation, spot work | Buy Now |
| Triple-Chip Wrap | 660 + 850 nm | Wearable belt | Hands-free targeted recovery | Buy Now |
| SUBRUN Panel | 660 + 850 nm | Panel (3 modes) | Minimum-cost entry | Buy Now |
Device availability and pricing change frequently. Confirm current specifications, reviews, and price at the link before buying.
At-Home Devices vs Professional Devices — What to Know
This is the most underdiscussed point in the consumer red light therapy market. The majority of muscle recovery RCTs cited above used clinical laser devices, not LED panels. According to the 2024 J Funct Morphol Kinesiol review (PMC11503318), laser light is coherent, monochromatic, and penetrates much deeper than the non-coherent, broader-spectrum light produced by LEDs. The review explicitly notes that LED devices are not subject to Federal laser product performance standards.
Practically: a consumer LED panel is not equivalent to the lasers that produced the strongest positive results. LED panels still appear to produce useful biological effects — research on LED-based PBM in athletes has reported reductions in fatigue markers and perceived soreness — but expect more modest effects than the trial headlines suggest, and budget accordingly.
Who Should Avoid Red Light Therapy?
Based on contraindications consistently listed across published reviews and the JAAD CME (2024 review):
- People with photosensitivity disorders (e.g., lupus, porphyria)
- Anyone taking photosensitizing medications — certain tetracyclines, fluoroquinolones, NSAIDs, retinoids, and St John's wort. Check with your prescriber.
- People with active skin cancers or untreated suspicious lesions in the treatment area
- Pregnant individuals — limited safety data, treat as precautionary
- People with active hyperthyroidism treating the neck — caution advised
- Epilepsy — flicker risk if device PWM frequency is low
Always use the goggles your device ships with, and do not stare into the diodes.
FAQ
Does red light therapy actually work for muscle recovery?
For pre-exercise application and late-phase DOMS, the evidence is meaningful. A 2025 meta-analysis of 19 RCTs (PubMed 40954632) found PBMT before exercise significantly reduced muscle soreness (low-certainty evidence). A separate 2025 network meta-analysis (PMC12178262) found PBMT held a significant edge over placebo at 24 h post-DOMS induction. Expect modest, real-world effects rather than dramatic ones.
When is the best time to use red light therapy — before or after a workout?
Before has the stronger evidence base. The 2025 pre-exercise meta-analysis (PubMed 40954632) is the most-replicated finding in the field. Post-exercise use is also studied but evidence is more mixed, with the 2025 DOMS meta-analysis (PMC12286287) showing benefits most clearly at 72–96 h after eccentric damage.
How long until I see results?
Most positive RCTs measured outcomes after single sessions for pre-exercise effects, but consumer-level perceived recovery typically takes 3–6 weeks of consistent use (3–5 sessions per week) before users notice clear differences. If you see no benefit at 8 weeks of disciplined use, the modality may not be a fit for your goals.
What wavelength is best for muscle recovery — 660 nm or 850 nm?
For muscle tissue specifically, 850 nm matters more because penetration depth is greater. The studied protocols typically use both — 660 nm for surface and superficial structures, 850 nm for deeper muscle tissue. NIR-heavy panels (like the Viconor's 1:2 red:NIR ratio) lean into this for recovery use.
Can I use red light therapy every day?
Daily use at recommended doses is generally safe. Most positive trials used 3–5 sessions per week rather than daily — there is a documented "biphasic dose response" in PBM literature where too much light can blunt effects. Follow manufacturer guidance on session length and distance.
Is there a difference between an at-home panel and a professional device?
Yes — and it is material. Professional devices used in most positive RCTs are lasers, which produce coherent monochromatic light that penetrates deeper than the LEDs in consumer panels (PMC11503318). Consumer LED panels still produce useful biological effects but expect more modest results than clinical-laser headlines suggest.
Does red light therapy reduce creatine kinase levels?
Several smaller trials have reported reductions in creatine kinase (CK) and other muscle damage biomarkers following PBM, but pooled effect sizes vary by protocol and the evidence is not yet robust enough to call this a settled finding. Treat CK reduction as a plausible mechanism, not a clinical certainty.
Who should not use red light therapy?
Pregnant individuals, people with photosensitivity disorders or on photosensitizing medications, anyone with active skin cancers in the treatment area, and people with epilepsy (where device flicker is a concern) should consult a clinician before use. See the contraindications section above.
Conclusion
After reading through PubMed and PMC studies through August 2025, the position is clear: red light therapy is a legitimate, modestly evidence-supported tool for muscle recovery — particularly when applied before exercise, with 660 nm + 850 nm, in the 120–300 J per zone range. It is not a substitute for sleep, nutrition, or progressive training. It is a credible adjunct.
For most people, the Hooga HG300 is the best place to start. If you want a higher-power option backed by deeper review data, the BestQool 105W is the natural step up. For targeted muscle work at a desk or on the couch, the Triple-Chip Wrap is the most practical wearable option.
Medical disclaimer: This article is for informational purposes only. Always consult a qualified healthcare provider before making changes to your health routine. In particular, consult a provider if you are pregnant, take photosensitizing medications, have a photosensitivity disorder, or have any active skin condition in the treatment area before starting red light therapy.
Product recommendations are based on independent research, device specifications, and published clinical evidence. No manufacturers paid for inclusion in this guide. Star ratings and availability change over time, so confirm current details at the link before buying.
See also: Red Light Therapy for Skin: What the Evidence Supports, Best Red Light Therapy Device for Home Use in 2026, What Is Mindful Living? A Clear Explanation for Beginners.
Sources
- Pre-exercise PBMT, NMES and IPC for muscle recovery — systematic review and meta-analysis, 19 RCTs (n=672). PubMed 40954632. https://pubmed.ncbi.nlm.nih.gov/40954632/
- Leal-Junior ECP, Lopes-Martins RAB, Bjordal JM. Clinical and scientific recommendations for PBMT in exercise performance enhancement and post-exercise recovery. PMC6546960. https://pmc.ncbi.nlm.nih.gov/articles/PMC6546960/
- Photobiomodulation as Medicine: LLLT for Acute Tissue Injury or Sport Performance Recovery. J Funct Morphol Kinesiol, 2024. PMC11503318. https://pmc.ncbi.nlm.nih.gov/articles/PMC11503318/
- Differences in the Effectiveness of Different Physical Therapy Modalities in the Treatment of DOMS: Systematic Review and Bayesian Network Meta-Analysis. J Pain Research, 2025. PMC12178262. https://pmc.ncbi.nlm.nih.gov/articles/PMC12178262/
- Effects of Photomodulation Therapy for Delayed Onset Muscle Soreness: Systematic Review and Meta-Analysis (14 studies, 660–950 nm). PMC12286287. https://pmc.ncbi.nlm.nih.gov/articles/PMC12286287/
- PBMT at 808 nm Does Not Improve Biceps Brachii Performance to Exhaustion and DOMS in Young Adult Women: Randomized Crossover Trial. PMC8222918. https://pmc.ncbi.nlm.nih.gov/articles/PMC8222918/
- Photobiomodulation CME overview, J Am Acad Dermatol, 2024. https://www.jaad.org/article/S0190-9622(24)00186-5/abstract

Marcus Thorne, PhD
A wellness researcher focused on what the evidence actually says.

